










COVID-19 from Community Medicine Perspective
COVID-19 bags its position to be one of the biggest pandemics known to humankind. Outbreak of COVID-19 as a pandemic in 2020 has impacted the lives of people globally in a huge manner. Living with the pandemic has become new normal now and people are trying to manage/revamp their lives in as normal a way as possible.
Epidemiology
- SARS-CoV-2 originated from China in December 2019 and spread rapidly to affect rest of the world over a period of 3-4 months. It produced a large cluster of pneumonia cases.
- WHO declared it a global pandemic on 11th March 2020. Maximum number of cases were recorded in USA followed by India and Brazil.
- The COVID-19 pandemic is the third recorded outbreak of a coronavirus, with the 2002 sudden acute respiratory syndrome (SARS, SARS-CoV-1 or SARS-CoV) and the 2012 Middle East respiratory syndrome (MERS or MERS-CoV) epidemics preceding it.
- The COVID-19 case fatality rate is challenging to evaluate, due to widespread variability in public health response and capacity, availability of treatment, national demography, viral variants, and prevalence of comorbidities.
- The mortality rate of COVID-19 is currently estimated to be between 2% and 4 %; however, some countries have a case fatality rate of less than 1%, while others (particularly poorer countries, and those whose healthcare systems have been overrun) have a case fatality rate as high as 25 %.
Causative Agent
COVID-19 is caused by the novel coronavirus SARS-COV-2. According to WHO, the incubation period of the virus is estimated to be between 2 and 14 days and on average 5.2 days. As per WHO, a very long incubation period could represent a double exposure.
Source: Data from Wuhan
Variants of SARS-CoV-2
The newer variants of the virus are classified into Variants of Interest (VoI) and Variants of Concern (VoC)
- Variants of Interest (VOI) have changed phenotypic properties compared to the known existing virus due to mutations that need further study
- Variants of Concern (VOC) are those strains of the virus that demonstrate changes in the form of Increased transmissibility, change in disease presentation or severity, change in our ability to control the virus using public health measures, or use of diagnostics, therapeutics, and vaccines.
| WHO label | Variant | Earliest documented samples | Date of designation |
| Alpha | B.1.1.7 | The United Kingdom,Sep-20 | 18-Dec-20 |
| Beta | B.1.351 | South Africa,May-20 | 18-Dec-20 |
| Gamma | P.1 | Brazil,Nov-20 | 11-Jan-21 |
| Delta | B.1.617.2 | India,Oct-20 | VOI: 4-Apr-2021 VOC: 11-May-2021 |
| Omicron* | B.1.1.529 | Multiple countries, Nov-2021 | VUM: 24-Nov-2021 VOC: 26-Nov-2021 |
Source: https://www.who.int/en/activities/tracking-SARS-CoV-2-variants/
Abbreviations: VOI: variant of interest; VOC: variant of concern; VUM: variant under monitoring.
Case Definition: Who Surveillance Guidelines
- Suspect Case
- A patient with acute respiratory illness (fever and at least one sign/symptom of respiratory disease, e.g., cough, shortness of breath), AND a history of travel to or residence in a location reporting community transmission of COVID-19 disease during the 14 days prior to symptom onset.
- OR A patient with any acute respiratory illness AND having been in contact with a confirmed or probable COVID-19 case in the last 14 days prior to symptom onset.
- OR A patient with severe acute respiratory illness (fever and at least one sign/symptom of respiratory disease, e.g., cough, shortness of breath; AND requiring hospitalization) AND in the absence of an alternative diagnosis that fully explains the clinical presentation.
- Probable Case
- A suspect case for whom testing for the COVID-19 virus is inconclusive; OR A suspect case for whom testing could not be performed for any reason
- Confirmed Case
- A person with laboratory confirmation of COVID-19 infection, irrespective of clinical signs and symptoms
Transmission
- According to research, the high affinity of the 2019-nCoV S for human ACE2 may function as a factor for human-to human transmission but further studies are needed to investigate this possibility.
- Solutions like: 62–71% ethanol, 50–100% isopropanol, 0.1% sodium hypochlorite, 0.5% hydrogen peroxide and 0.2–7.5% povidone-iodine may be used for disinfection.
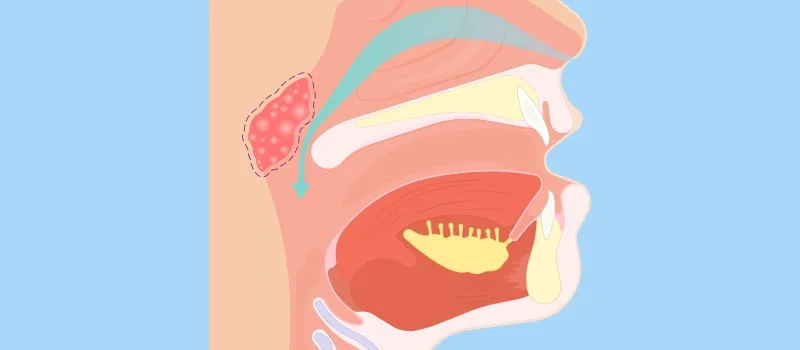
Droplet Transmission
- Droplet transmission occurs when a person is in close contact (within 1 m) with someone who has respiratory symptoms.
- Therefore, at risk of having his/her mucosae (mouth and nose) or conjunctiva (eyes) exposed to potentially infective respiratory droplets.6
Contact Transmission
- Transmission may also occur through fomites in the immediate environment around the infected person.
- Therefore, transmission of the COVID-19 virus can occur by direct contact with infected people and indirect contact with surfaces in the immediate environment or with objects used on the infected person.
- Frequent hand hygiene following potential contact exposure is crucial to prevent this type of transmission.
Aerosol Transmission
- Spread of the infected droplet nuclei beyond one meter – not documented yet.
- Specific settings in which aerosol-generating procedures are performed (e.g., endotracheal intubation), aerosol transmission of the COVID-19 virus may be possible.
- Use of N95 respirator – important to prevent this type of transmission.
Viral Load Dynamics and Duration of Illness
- In the respiratory tract, peak SARS-CoV-2 load is observed at the time of symptom onset or in the first week of illness, which indicates the highest infectiousness potential just before or within the first five days of symptom onset.
- After the initial exposure, patients typically develop symptoms within 5-6 days (incubation period). The viral load peaks in the first week of infection, declines thereafter gradually, while the antibody response gradually increases and is often detectable by day fourteen.
Clinical Manifestations
- Typically results in flu-like symptoms including fever and cough
- Begins with a fever, followed by a dry cough and after a week result in shortness of breath (approx. 20% of patients require hospital treatment)
- Sneezing, sore throat, and running nose (rarely).
- Sneezing, stuffy nose, and sore throat are usually signs of a cold
- Pre-existing illnesses: Patients with pre-existing conditions like cardiovascular disease, diabetes, chronic respiratory disease, and hypertension are more vulnerable to the disease
- It may present with mild, moderate, or severe illness that includes severe pneumonia, acute respiratory distress syndrome, sepsis, and septic shock.
- Mild to moderate disease: 80% includes pneumonia and non-pneumonia cases
- Severe disease: 13.8% includes dyspnea, respiratory frequency ≥30/minute, blood oxygen saturation ≤93%, PaO2/FiO2 ratio <300, and/or lung infiltrates >50% of the lung field within 24–48 hours
- Critical cases: 6.1% (respiratory failure, septic shock, and/or multiple organ dysfunction/failure).
Protection of Susceptible Host
- Virus vaccines: The virus itself is used in a weakened or inactivated form. Types: Weakened or inactivated.
- Viral-vector vaccines: A weakened virus, such as adenovirus or measles, is genetically engineered to produce coronavirus proteins in the body. Types: Replicating viral vector and non-replicating viral vector.
- Nucleic-acid vaccines: Nucleic acid is inserted into human cells, which then produce copies of the virus protein which produces an immune response. Types: DNA vaccine and RNA vaccine.
- Protein-based vaccines: Virus protein fragments or protein shells are injected directly into the body. Types: Protein subunit vaccines and virus-like particle vaccines
- Vaccines currently in use in India:
- Two vaccines are currently licensed for use in India, i.e., Covishield and Covaxin. Both the vaccines have 100% efficacy against severe COVID-19, hospitalization, and death. Studies to confirm efficacy against COVID-19 infection and reduction of transmission are ongoing. Other vaccines licensed in India are Sputnik V from Russia to be manufactured by Serum Institute and Moderna from the USA, to be imported by Cipla.